
Most conversations about skin aging start with collagen, retinoids, or sun damage. Few start with the immune system. But a growing body of research places chronic, low-grade immune activation, not only UV exposure or the passage of time, at the center of why skin ages, breaks out, and turns red or reactive.
The term for this is inflammaging: a slow-burning, whole-body inflammatory state that intensifies with age and with a handful of everyday exposures. It is not a wellness buzzword. It was defined by immunologists over two decades ago and has since become one of the most active areas of aging research, with a growing focus on exactly what it does to skin.
Your Skin Has Its Own Immune System
Skin is usually described as a barrier, a wall that keeps the outside world out. That description undersells it. Skin is also one of the largest immune organs in the body, populated with resident immune cells that constantly monitor for damage, pathogens, and irritants.
Keratinocytes, the main cells of the outer epidermis, are not passive bricks. They produce cytokines and antimicrobial peptides directly in response to UV exposure, pollutants, and microbial contact. Langerhans cells, a type of dendritic cell embedded in the epidermis, continuously sample the environment and coordinate immune responses. Mast cells, macrophages, and circulating immune cells including neutrophils are recruited into skin tissue whenever a threat is detected.
This matters because it means every visible skin concern, acne, redness, dullness, fine lines, has an immune signature underneath it. Ingredients and skincare routines work largely on the surface. The immune biology helps explain why the same product can behave so differently on two people, and why stress, sleep, and diet show up on the face.
Acute Inflammation: The Immune Response Working as Intended
Before looking at what goes wrong, it helps to see what inflammation looks like when it is working correctly. Acute inflammation is the reason a blemish, a sunburn, or a small cut heals instead of simply staying damaged.
When skin is injured, exposed to bacteria, or hit with a burst of UV radiation, resident immune cells release signaling molecules that widen local blood vessels and recruit neutrophils, the most abundant white blood cell in circulation and the first responders of the innate immune system. Neutrophils arrive within minutes to hours, engulf bacteria and debris through phagocytosis, and release reactive oxygen species and enzymes that help clear the threat.
This produces the classic signs of inflammation: redness, heat, swelling, and sometimes pain. It looks alarming, but it is protective. Once the threat is cleared, the response resolves. Neutrophils undergo programmed cell death, macrophages clear the remains, and tissue repair begins. A well-functioning acute inflammatory response is fast, proportional, and temporary.
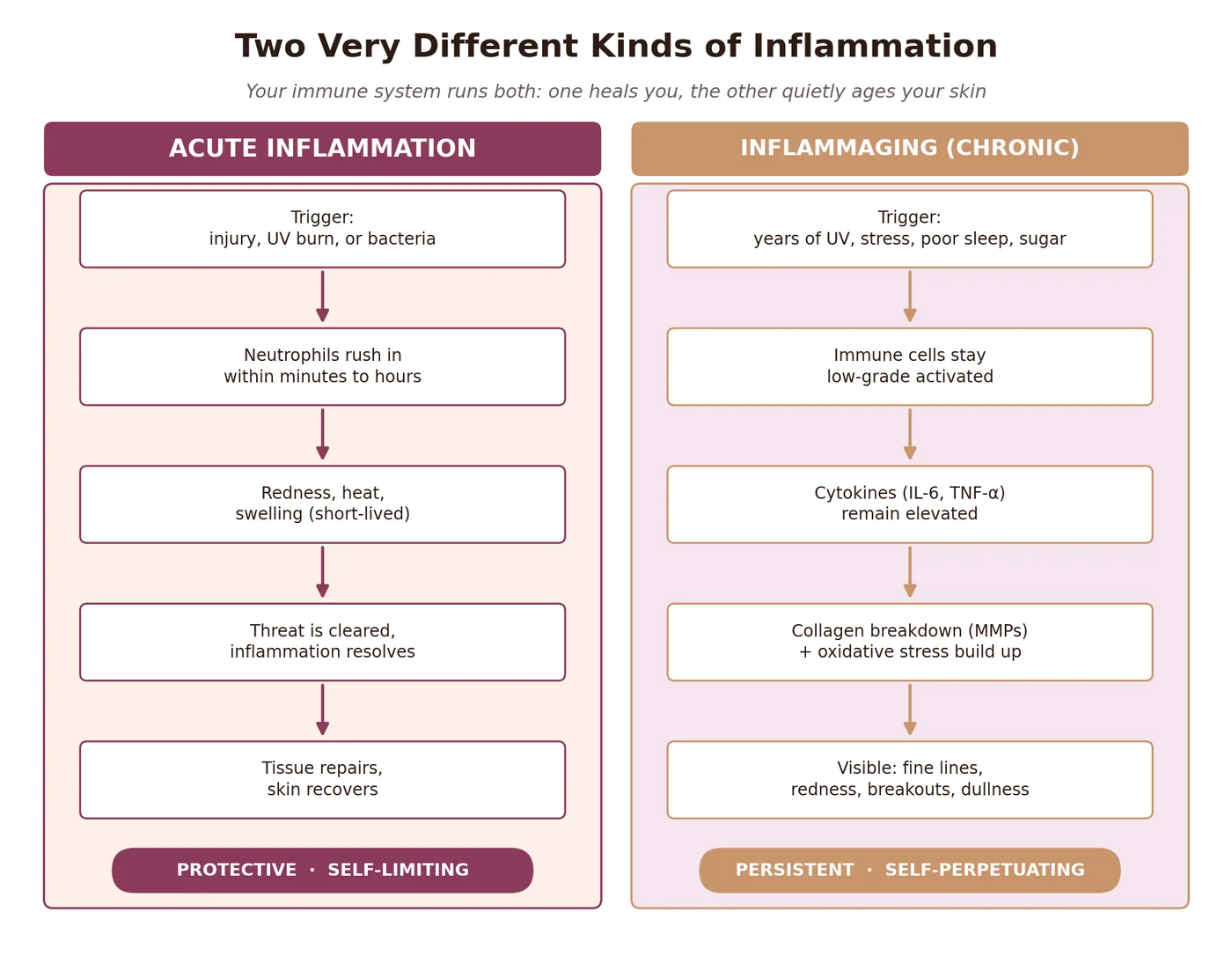
Inflammaging is what happens when this system stops turning off.
When Inflammation Becomes Chronic: Understanding Inflammaging
The term inflammaging was introduced in 2000 by immunologist Claudio Franceschi and colleagues, who observed that aging is consistently accompanied by a low-grade, chronic, systemic inflammatory state, distinct from the acute response described above.
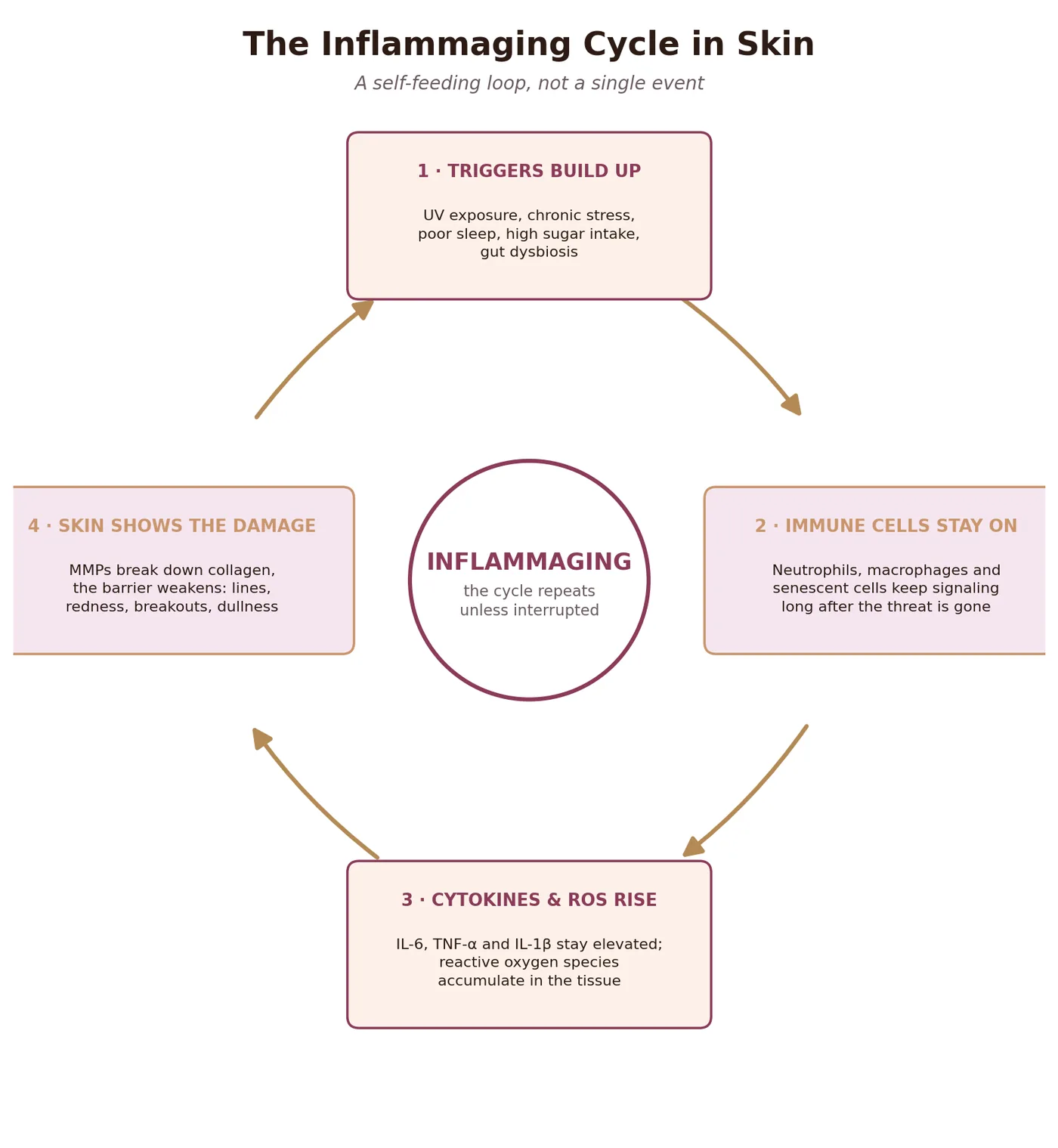
Where acute inflammation is fast and self-limiting, inflammaging is slow, persistent, and largely silent. It is characterized by chronically elevated pro-inflammatory cytokines, including interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-\u03b1), and interleukin-1 beta (IL-1\u03b2), circulating at low but continuously raised levels rather than the sharp spike-and-resolve pattern of a healthy acute response.
A 2025 review examining the cutaneous side of inflammaging specifically found that skin-resident immune cells are reshaped by this process over time. Langerhans cells decline in number and function under sustained low-grade inflammation, weakening the skin’s own immune surveillance, while skin-resident T cell populations shift toward a more inflammatory local balance.
One driver behind this is cellular senescence. Cells that stop dividing but do not die, senescent cells, accumulate with age and chronic stress, and they secrete a mix of inflammatory cytokines and tissue-degrading enzymes known as the senescence-associated secretory phenotype, or SASP. This creates a feedback loop: senescent cells generate inflammation, and inflammation promotes further cellular senescence.
The Estrogen Connection: Why It Often Accelerates at Perimenopause
Inflammaging affects everyone, but not equally and not at the same pace. Estrogen has direct anti-inflammatory effects, including suppressing pro-inflammatory signaling within immune cells and supporting vascular function. As estrogen declines through perimenopause and menopause, this brake weakens.
A study measuring circulating interleukin-6 across reproductive stages in healthy, non-obese women found that postmenopausal participants had measurably higher IL-6 levels than premenopausal women of similar age and body composition, with a statistically significant interaction between chronological age and menopausal status. In plain terms, the hormonal transition itself, not only the passage of time, appears to contribute to the shift.
This is one of the more plausible biological explanations for why some women notice a distinct change in skin behavior around perimenopause, more redness, slower recovery after irritation, increased reactivity, beyond what chronological aging alone would predict. It is also a specific, evidence-grounded reason why inflammation-focused strategies may become more relevant, not less, during and after this transition. BioFlowBeauty’s piece on hormonal health covers the broader hormonal picture in more depth.
How Inflammaging Shows Up in Your Skin
Inflammaging is not an abstract, internal process. It has specific, visible consequences, and the mechanisms behind several common concerns are better understood as immune stories than purely cosmetic ones.
Acne Is an Immune Event, Not Just Clogged Pores
Acne is conventionally explained through clogged pores, excess sebum, and bacteria. All of that is true, but the visible, inflamed lesions, red and painful bumps rather than simple blackheads, are driven substantially by neutrophils.
When a follicle wall ruptures, neutrophils infiltrate the area and generate reactive oxygen species as part of their normal antimicrobial function. Research measuring hydrogen peroxide output found that patients with inflammatory acne lesions had significantly higher neutrophil-generated hydrogen peroxide than patients with only comedonal acne (blackheads and whiteheads) or healthy controls, and that reducing this neutrophil activity with oral minocycline tracked closely with reduced inflammatory activity in the lesions themselves.
This reframes inflammatory acne as less of a hygiene or clogged-pore problem and more of a localized, overactive innate immune response. It is also why calming approaches, not only pore-clearing ones, matter specifically for the inflamed, painful lesions rather than blackheads.
Photoaging Is Largely Inflammation-Driven Collagen Loss
Sun damage is usually framed as direct damage from UV radiation. Mechanistically, a large share of it runs through the immune system. UV exposure triggers keratinocytes and dermal fibroblasts to generate reactive oxygen species, which activate inflammatory signaling pathways and drive the expression of matrix metalloproteinases (MMPs), enzymes that break down collagen and elastin in the dermis.
A single UV exposure sufficient to cause mild redness measurably suppresses new collagen production for roughly 24 hours and raises MMP activity that degrades existing collagen for days afterward. Repeated over years, this inflammatory cycle of collagen breakdown outpacing collagen synthesis is a central mechanism behind photoaging, arguably more so than UV radiation simply drying out the skin.
This is also why chronic, low-grade inflammation from non-UV sources, poor sleep, high sugar intake, chronic stress, can compound photoaging even in skin that gets reasonable sun protection. The MMP pathway responds to inflammatory signaling broadly, not only to UV specifically. BioFlowBeauty’s skincare science article covers retinoids and antioxidants, both of which intersect with this same pathway.
Redness, Sensitivity, and a Weakened Barrier
Persistent facial redness, whether rosacea, general reactivity, or skin that seems to flush at the slightest provocation, reflects a lower threshold for immune activation. In this state, mast cells and the local vasculature respond more readily to triggers, heat, spicy food, certain actives, that would not provoke a visible response in calmer skin.
A weakened skin barrier and chronic low-grade inflammation tend to reinforce each other. Barrier dysfunction lets more irritants and microbes reach immune cells deeper in the epidermis, prompting more inflammatory signaling, which in turn further impairs barrier repair. Breaking this cycle usually means addressing the barrier and the underlying inflammatory drivers together, not one in isolation.

What Drives Chronic Inflammation
Several everyday, modifiable factors keep the inflammaging process switched on. None of them are exotic, and several overlap with hormones and the gut microbiome, because inflammation, hormones, and the microbiome are deeply intertwined systems rather than separate ones.
UV exposure is the most direct, best-documented driver of skin-specific inflammaging, through the MMP and oxidative stress pathway described above. Daily broad-spectrum sun protection remains the single highest-leverage intervention available.
Poor sleep measurably raises circulating inflammatory markers. A 2026 meta-analysis of experimental sleep deprivation studies found that multiple nights of restricted sleep produced a significant increase in both IL-6 and C-reactive protein (CRP), two of the core markers associated with inflammaging, while a single night of poor sleep did not produce the same measurable effect. Consistency appears to matter more than any one bad night.
Chronic psychological stress activates the hypothalamic-pituitary-adrenal axis, and sustained cortisol elevation has direct effects on immune cell behavior and barrier repair.
Gut dysbiosis contributes to systemic inflammation through increased intestinal permeability, allowing bacterial components to reach circulation and activate immune signaling at a low, continuous level. BioFlowBeauty’s piece on gut health and hormones covers this connection in more depth.
Diet, specifically high intake of refined sugar and ultra-processed foods, promotes the formation of advanced glycation end products, which bind to collagen and other structural proteins and provoke inflammatory signaling directly in tissue, skin included.
Evidence-Based Ways to Calm Chronic Inflammation
The encouraging part of inflammaging research is that, unlike purely genetic aging processes, most of its known drivers are modifiable.
Prioritize sun protection daily, not only when heading outdoors intentionally. Incidental UV exposure accumulates and remains one of the clearest, most direct drivers of skin-specific inflammaging.
Protect sleep consistency over chasing an occasional perfect night. The evidence points to cumulative, multi-night restriction as the trigger for measurable inflammatory increases, which means a consistent pattern matters more than any single late night.
Increase dietary omega-3 intake. A review of omega-3 fatty acids and skin disease found that EPA and DHA are converted into specialized pro-resolving mediators, including resolvins and protectins, that actively help inflammation resolve rather than simply suppressing it, with supporting evidence across several inflammatory skin conditions. Fatty fish, walnuts, flaxseed, and algae-based supplements are practical sources.

Support the gut microbiome, since intestinal permeability is one of the upstream contributors to systemic inflammatory tone. Fiber intake and fermented foods remain the two interventions with the most consistent evidence here.
Manage chronic stress through whatever method is sustainable. The mechanism runs through cortisol and the HPA axis, but the intervention does not need to be complicated to be effective.
Consider topical actives with genuine anti-inflammatory evidence, including niacinamide and centella asiatica, both covered in more depth in BioFlowBeauty’s skincare science article.
None of these interventions work by suppressing the immune system. They work by reducing the chronic, low-grade triggers that keep it switched on longer than it needs to be.
What to Watch For
Inflammaging develops gradually, which makes it easy to miss until the visible signs accumulate. A few patterns are worth paying attention to.
Skin that feels warm, tight, or reactive most of the time, not only after a specific trigger, may reflect a lower activation threshold consistent with chronic low-grade inflammation.
Persistent redness that never fully resolves between flare-ups, rather than clear skin punctuated by occasional irritation, suggests the inflammatory baseline itself has shifted.
Inflammatory acne that responds poorly to standard pore-focused treatment may benefit from addressing systemic inflammatory drivers, sleep, stress, diet, alongside topical treatment rather than instead of it.
Skin aging that seems to be progressing faster than sun exposure alone would explain is worth examining through the lens of sleep, stress, and diet, not only skincare products.
These patterns do not replace a dermatology consultation for persistent or severe skin concerns, but they offer a more complete way of thinking about what skin is actually responding to.
References:
- Franceschi C, Bonaf\u00e8 M, Valensin S, Olivieri F, De Luca M, Ottaviani E, De Benedictis G. (2000). Inflamm-aging. An evolutionary perspective on immunosenescence. Annals of the New York Academy of Sciences, 908, 244-254. PubMed
- Karpuzoglu E, Holladay SD, Gogal RM. (2025). Inflammaging: triggers, molecular mechanisms, immunological consequences, sex differences, and cutaneous manifestations. Frontiers in Immunology, 16. DOI
- Kim OY, Chae JS, Paik JK, Seo HS, Jang Y, Cavaillon JM, Lee JH. (2012). Effects of aging and menopause on serum interleukin-6 levels and peripheral blood mononuclear cell cytokine production in healthy nonobese women. Age, 34(2), 415-425. DOI
- Akamatsu H, Horio T, Hattori K. (2003). Increased hydrogen peroxide generation by neutrophils from patients with acne inflammation. International Journal of Dermatology, 42(5), 366-369. PubMed
- Pittayapruek P, Meephansan J, Prapapan O, Komine M, Ohtsuki M. (2016). Role of Matrix Metalloproteinases in Photoaging and Photocarcinogenesis. International Journal of Molecular Sciences, 17(6), 868. PubMed
- Ballesio A, Fiori V, Lombardo C. (2026). Effects of Experimental Sleep Deprivation on Peripheral Inflammation: An Updated Meta-Analysis of Human Studies. Journal of Sleep Research, 35(1), e70099. PubMed
- Sawada Y, Saito-Sasaki N, Nakamura M. (2021). Omega 3 Fatty Acid and Skin Diseases. Frontiers in Immunology, 11, 623052. PubMed
For related topics, explore BioFlowBeauty’s posts on skincare science and gut health and women’s hormones, which cover the barrier and microbiome dimensions of this same inflammation story in more depth.